

Meeting overview
The 2026 ASCO Annual Meeting brought together more than 35,000 oncology professionals from around the world at McCormick Place in Chicago, organized around President Dr. Eric Small's theme: The Science and Practice of Translation: Improving Cancer Outcomes Worldwide.
While major clinical breakthroughs in lymphoma, breast cancer, prostate cancer, and lung cancer dominated the plenary sessions, a parallel and increasingly prominent thread ran through the entire meeting: AI and informatics are no longer peripheral topics, they are central to the future of oncology.
Significant IT & AI findings
1. AI is formally embedded across every disease track
The ASCO scientific program committee built AI as an explicit submission subcategory across virtually every disease area, including breast cancer, CNS tumors, and a dedicated Care Delivery track. This structural choice signals that AI has moved from a novelty session to a core scientific category.
2. Multimodal AI for digital pathology risk stratification
A poster session on prostate cancer presented results evaluating image-only and multimodal AI (MMAI) digital pathology biomarkers for risk stratification across standard localized prostate cancer management strategies. There is growing interest in AI-based pathology platforms capable of extracting additional prognostic information directly from routine hematoxylin and eosin slides. This is information that goes beyond what conventional clinicopathologic variables like Gleason grade, PSA, and tumor stage can provide.
3. A multiagent AI system for first-line NSCLC immunotherapy decisions
This was arguably the most significant IT finding with direct agentic AI implications. Researchers built a multiagent system trained with medical knowledge and web search access that gathered patient data, including electronic health records, CT imaging, histology slides, lab work, and molecular reports, to recommend first-line immunotherapy for non-small cell lung cancer. The system output a set of key findings, a rationale for its recommendation, and a treatment plan, and identified possible ambiguities and contradictions. The system produced correct statements 72% of the time as evaluated by four specialized oncologists, and recommendations were found to be helpful 72% of the time and complete 91% of the time.
Harvard/Mass General Brigham's Dr. Danielle Bitterman commented directly on the significance: agentic AI. When AI models such as large language models have "agency" to interact with each other and use digital tools within multistep workflows, they can enable AI to conduct more complex, high-order clinical tasks. This study, although small and limited to a single institution, is an exciting proof-of-concept for agentic AI for clinical decision support in cancer immunotherapy, where treatment decision-making often requires contextual reasoning.
4. The patient-facing AI information gap
A cross-sectional analysis presented at ASCO 2026 found that online resources for patients about AI and cancer care are severely lacking: existing webpages and videos are largely of low quality, difficult to read, and frequently omit the risks of AI use. The study highlighted a major opportunity, noting that AI is increasingly being used by patients to understand their diagnosis, treatment options, and prognosis, yet available information fails to meet patient needs.
5. ASCO launches dedicated AI platform
In February 2026, ASCO and Conexiant launched ASCO AI in Oncology (ascoai.org), a digital platform dedicated to understanding how AI is impacting cancer care. The platform covers topics including Diagnostics & Imaging, Decision-Making Support, Prognostic and Predictive Models, and Drug Discovery and Clinical Trials.
6. The regulatory frontier: autonomous AI prescribing
As of January 2026, Utah became the first state to launch a pilot program allowing an autonomous AI health platform to independently renew certain prescription medications without a human doctor's review. This raised urgent questions about whether oncology needs guardrails to ensure a machine isn't managing cancer medications without oncologist oversight.
7. AI in clinical trials: from promise to execution
The conversation around AI at ASCO 2026 has shifted from what AI could do to what it is already doing. Organizations are moving beyond isolated tools and pilot projects toward integrated approaches that connect data, AI, and workflows to deliver measurable outcomes. This marks a transition from experimentation to execution. Agentic AI workflows that automate multi-step processes, and platforms that connect insights directly to execution, were featured prominently.
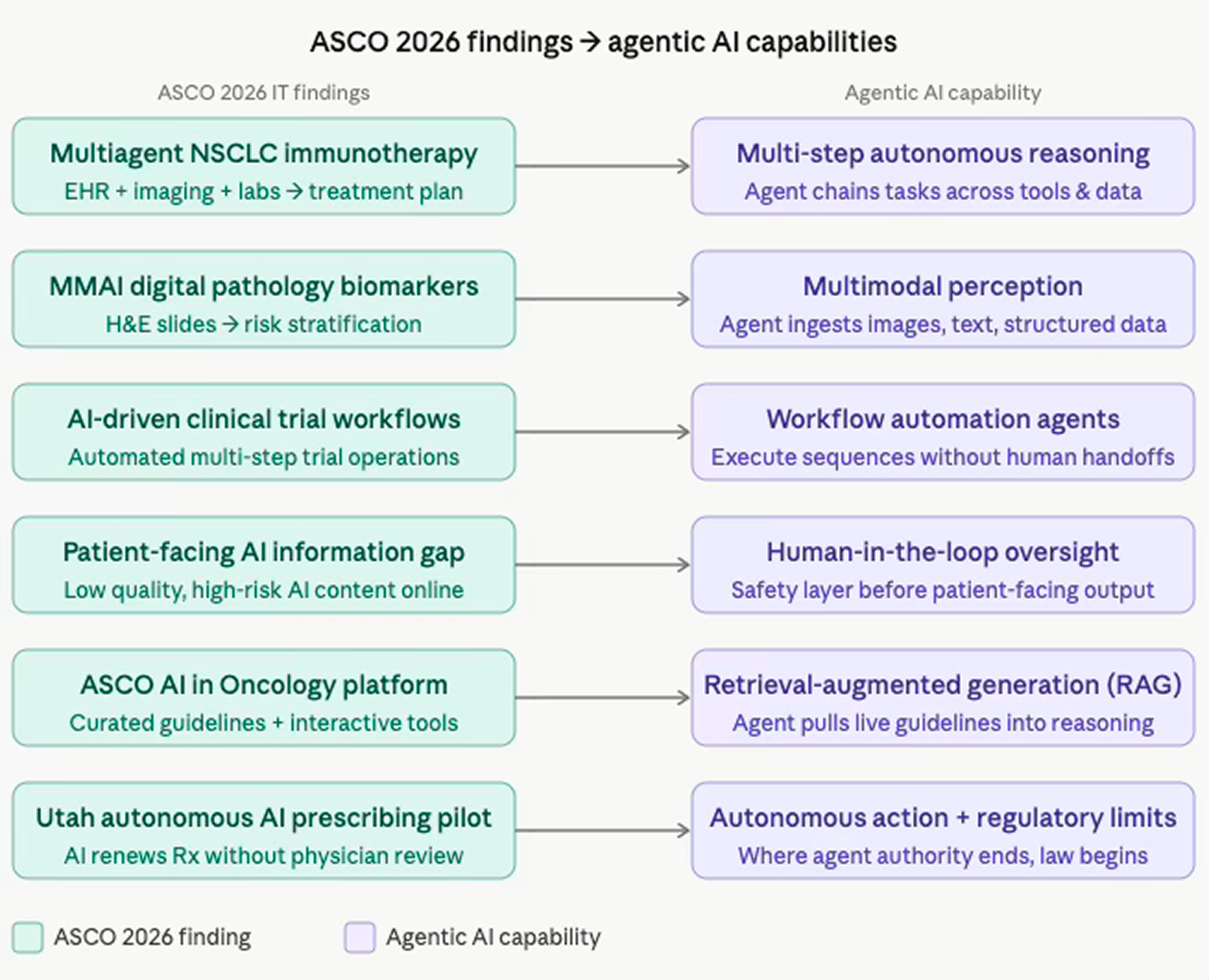
Connecting the findings to agentic AI
The diagram below summarizes how each finding maps to the core capabilities of agentic AI systems:
What this means for agentic AI in oncology
The through-line across all these findings is a clear trajectory: oncology is moving from AI as a passive analytical tool toward AI as an active, reasoning participant in clinical workflows. Several patterns are worth highlighting:
Multimodal data integration is the new baseline. The NSCLC multiagent study demonstrates that future oncology agents won't just read text. The agents will also ingest CT scans, pathology slides, lab values, and molecular reports simultaneously, synthesizing across modalities before making a recommendation. The multiagent architecture combined a React agent with RAG-based document querying, vision-language models for histology and radiology, and survival prediction tools, which are all orchestrated autonomously to output a complete treatment rationale. This is the template for what agentic AI in oncology will look like.
The "correctness ceiling" problem is real. At 72% accuracy, the NSCLC system is promising but not yet deployable without oversight. Researchers are working to enhance the trustworthiness of this system by introducing human-in-the-loop approaches, which maps directly to the core design principle of responsible agentic AI: keep a human in the decision loop, especially at high-stakes junctions.
From isolated models to integrated agents. ASCO's leadership identified three distinct fronts where AI is having meaningful impact: office operations and administrative automation, clinical care decision-making, and research innovation including drug discovery, molecular design, and clinical trial enrollment. Each of these corresponds to a tier of agentic complexity, from simple task automation to multi-step strategic reasoning.
The equity and literacy gap is a deployment risk. With patients already using AI to understand their diagnoses and treatment options, yet available information being largely low-quality and omitting risks, agentic systems that reach patients directly will need robust safeguards. These safeguards are not just to ensure clinical accuracy, but also explainability, equity auditing, and literacy-appropriate outputs.
Regulatory terrain is being defined in real time. The Utah autonomous prescribing pilot is a harbinger. The real question is how AI tools compare to current standards of cancer care, and the consensus emerging is that they will raise quality. Still, guardrails will be needed to ensure autonomous systems don't manage cancer medications without oncologist awareness. Agentic AI developers building for oncology must treat regulatory constraint not as an obstacle but as a core design parameter.
In short, ASCO 2026 confirmed that the oncology field is not waiting for agentic AI. It is actively building it, testing it in patients, and debating where its authority should begin and end.









